Pharmacology 1 - Unit 3
Syllabus
2. Pharmacology of drugs acting on peripheral nervous system
- Organization and function of ANS.
- Neurohumoral transmission,co-transmission and classification of neurotransmitters.
- Parasympathomimetics, Parasympatholytics, Sympathomimetics, sympatholytics.
- Neuromuscular blocking agents and skeletal muscle relaxants (peripheral).
- Local anesthetic agents.
- Drugs used in myasthenia gravis and glaucoma
Scroll to Download
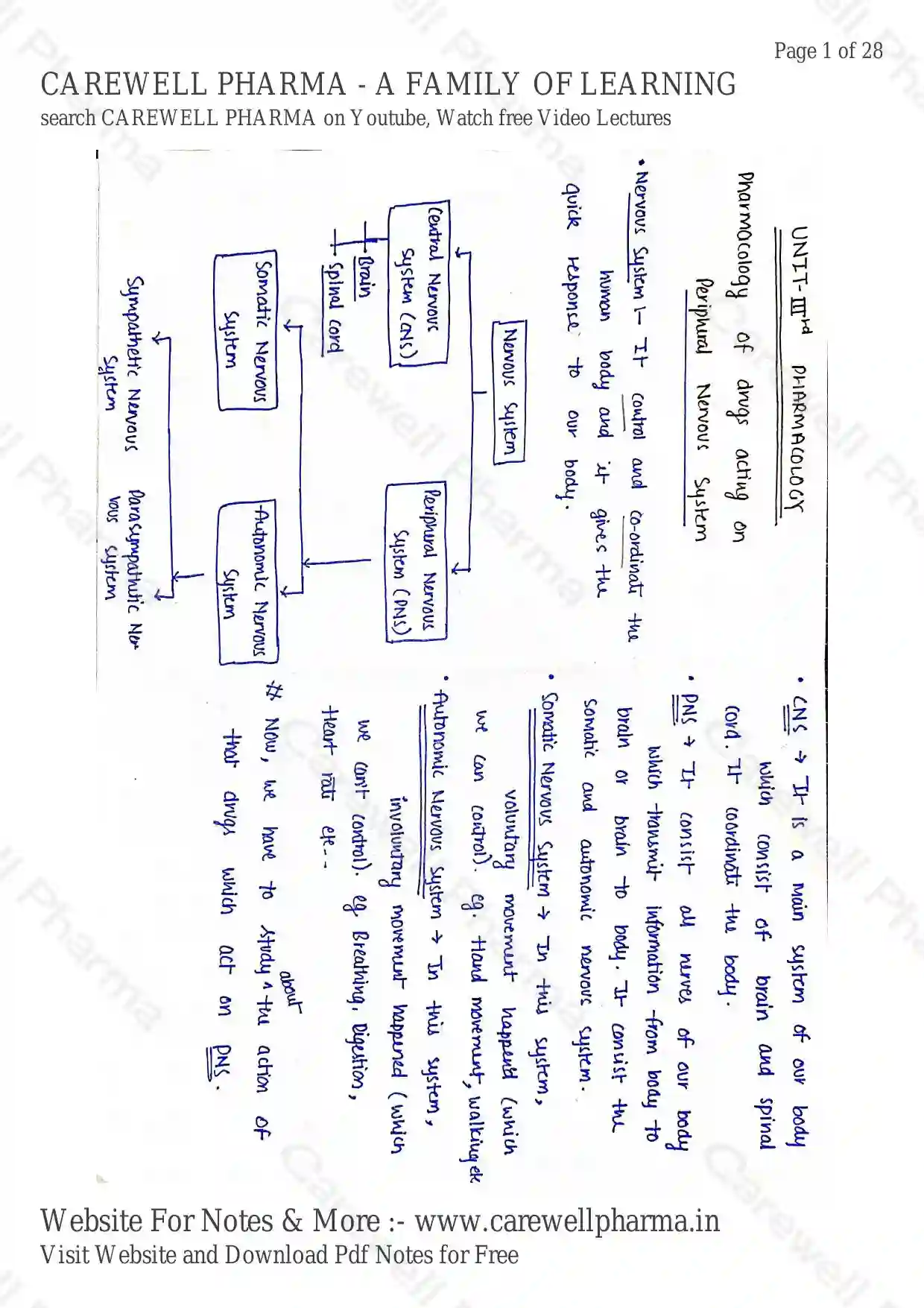
UNIT-III PHARMACOLOGY
Pharmacology of drugs acting on Peripheral Nervous System
Nervous System
It control and co-ordinate the human body and it gives the quick response to our body.
Nervous System
- Central Nervous System (CNS)
- Brain
- Spinal cord
- Peripheral Nervous System (PNS)
- Somatic Nervous System
- Autonomic Nervous System
- Sympathetic Nervous System
- Parasympathetic Nervous system
CNS
It is a main system of our body which consist of brain and spinal cord. It coordinate the body.
PNS
It consist all nerves of our body which transmit information from body to brain or brain to body. It consist the Somatic and autonomic nervous system.
Somatic Nervous System : In this system, voluntary movement happen'd (which we can control). eg. Hand movement, walking etc.
Autonomic Nervous system : In this system, involuntary movement happened (which we can't control). eg Breathing, Digestion, Heart rate etc--
Now, we have to study about the action of that drugs which act on PNS.
Syllabus
a). Organization and function of ANS.
b) Neurohumoral transmission, co-transmission and classification of neurotransmitter.
c) Parasympathomimetics, Parasympatholytics, Sympathomimetics, Sympatholytics.
d) Neuromuscular blocking agent and skeletal Muscle relaxants (peripheral).
e) Local anesthetic agents.
f) Drugs used in myasthenia gravis and glaucoma.
1) Organisation and function of ANS
ANS
Autonomic Nervous System
It involves involuntary responses (movement) of our body.
- It Further divided into two parts:
i).Sympathetic N.S.
ii). Parasympathetic N.S
1) Sympathetic Nervous System
- fear fight flight
- Those system which Activate in condition of fight/flight situation (Abnormal sitution) of body and maintain the body active in abnormal sitution.
- example - Increases heart rate, decease digestion rate etc.
ii) Parasympathetic Nervous system
- Rest and Digest condition
- In this, our body come back to normal condition after any abnormal sitution. Also help to maintain the homeostasis of body.
- example increase digestion rate and normal heart rate etc...
- Both system are motory function of body.
- Both system are important to maintain the homeostasis and motory function of body work of our body.
Different b/w Symapathetic & Parasympathetic system
| Sympathetic Nervous System | Para sympathetic Nervous system |
|---|---|
| • Involved in the fight or flight response | • Involved in maintaining homeostasis and also, permits the rest and digest response |
| • prepare the body for any potential danger. increase heartbeat, Muscles tense up, pupil dilate | • to bring the body to a state of calm. |
| • Saliva Secretion is inhibited | • Reduces heartbeat, muscle relaxes. • pupil contract • Saliva secretion increases, digestion increases |
| Neurotransmitter release Adrenaline and nor-adrenaline | Neurotransmitter release Acetylcholine |
NEUROHUMORAL TRANSMISSION
Neuro (Nerve / Neuron) + humoral (Chemical messenger)
- It is the process of transfer of any message or signal from one neuron to another neuron with the help of any chemical messenger (neurotransmitter, hormones, etc).
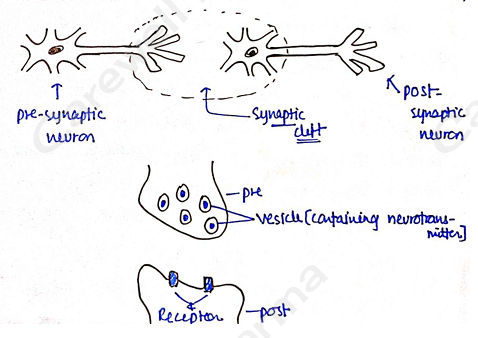
- For this purpose, firstly neurotransmitter is synthesized and stored in vesicles in nerve terminals.
- Now, Neurohumoral transmission involves following steps:
i) Impulse Conductance
ii) Transmitter release
iii) Transmitter action on post Junctional membrane iv) Post Junctional activity
v) Termination of transmitter action.
i) Impulse conductance
- In this step, firstly Impulse is generated by the process of "Action potential".
- At resting state (when nerve impulse is not transmitted from neuron), Resting trans-membrane potential is -70 mv.
- ion have high concentration at outside the cell and more (+)ve charge at outside the plasma membrane.
- ion have high concentration at inside the cell and more (-)ve charge at inside the plasma membrane.
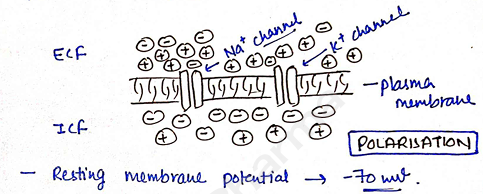
- Resting membrane potential -70 ml.
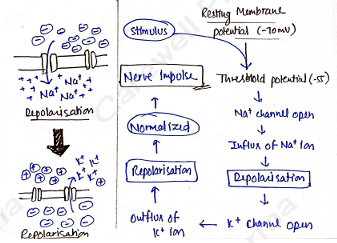
Depolarisation - When any kind of stimulus detected, then it changes the Resting Membrane potential to less potential (increases).
- If stimulus change resting potential (-70mV) to (-55mV) then it is called threshold potential.
- Threshold potential open ion channel.
- ion enters inside the cell and (+) ve charge produce inside the cell and (-)ve at outside the cell and it is called depolarisation.
Repolarisation - Stimulus continues increase the potential, now when potential reach at (+20 mv to + 30mV) it open ion channel and ion move outside the cells. This Normalized the potential.
- The ionic distribution is normalized during the refractory period by the activation of pump.
- The cycle of depolarisation and repolarisation is called Action Potential.
- These action potential works 1000 times in one second.
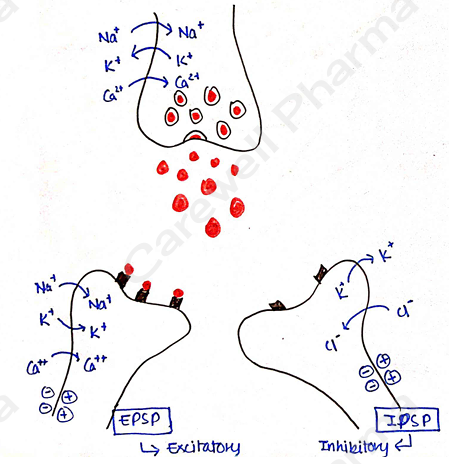
ii) Transmitter release
Nerve Impulse promotes fusion of vascular and axonal membrane, which through entry fluidized membranes. promotes exocytosis (transmitter release from vesicle) in synaptic cleft.
iii) Transmitter action on postjunction membrane
The transmitter release and attached with specific receptor and depending on nature it Induce two type of action
EPSP [Excitatory post-synaptic potential] increase in permeability to all cation or channel open Influx of ion Depolarisation Influx cause depolarisation followed by efflux.
IPSP [Inhibitory post synaptic potential] increase in permeability to smaller ion or anions. and moveys in, resulting move out Hyperpolarisation. Resist depolarizing stimuli.
iv) Post Junctional activity
- Nerve impulse, contraction in muscle, secretion in glands.
v) Termination of transmitter action
- Neurotransmitter is degraded locally or any other mechanism.
- It can also be degraded by enzymatic action.
eg. Acetylcholine degraded by cholinesterase.
Co-Transmission
- Peripheral and Central nervous system release more than one active substance when stimulated.
Definition : co-transmission is the release of several types of neurotransmitter from a single nerve terminal.
Co-transmitter : is a chemical substance that is released along with primary neurotransmitter.
examples
- In autonomic nervous system
- Primary neurotransmitter Ach, NA
- Co-transmitter are
- Purines:- ATP, Adenosine
- Peptides:- Vaso intestinal peptide (VIP)
- Nitric oxide, Prostaglandins (PG)
- On release of Acetylcholine (Ach), Vasoactive intestinal peptide (VIP) Co-transmitter release.
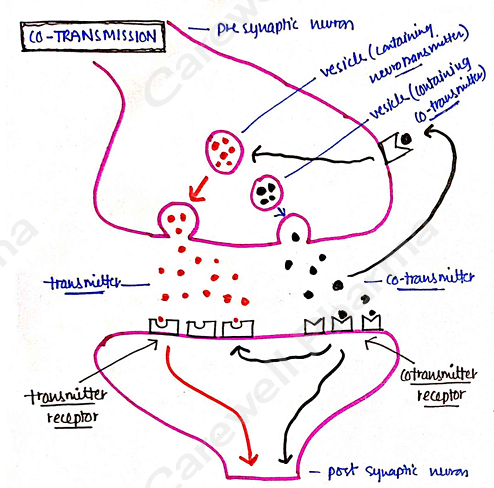
- Cotransmitter is stored with primary transmitter vesicle or in different (separate) vesicle.
Function
i) enhance or regulate presynaptic release of primary neurotransmitter.
ii) Modulate post-synaptic sensitivity of primary neurotransmitter.
iii) serve as a alternate to primary neurotransmitter.
Classification of Neurotransmitters
Neurotransmitter
These are chemical messenger that transmit signal from a neuron to a target cell across a synapse.
- Target cells may be a other neuron or some other kind of cell such as muscles or glands.
- These are stored into synaptic vesicle in pre-synaptic neurons.
Neurotransmitter bind RECEPTOR ACTION
- They can be classified as either excitatory or inhibitory.
Excitatory : Activate receptor on post-synaptic Membrane and enhance the effect of the actionat potential (increase activity).
Inhibitory : decrease the activity of transmitter or receptor. (decrease the effect of the action potential.
Some neurotransmitter show both type of activity.
| Excitatory | Inhibitory | Both |
|---|---|---|
| • Acetylcholine • Adrenaline • Nor-adrenaline • Histamine • Glutamate | • GABA • Serotonine • Dopamine | • Acetylcholine • Dopamine • Nor-adrenaline |
following major neurotransmitter with their functions
- Acetylcholine (Learning) : Involved in thought, learning, and memory.
- It activate muscle contraction in the body and is also associated with attention and awekening.
- Adrenaline (fight or flight) : It is primarily released by the adrenal gland, but some neurons may secrete it as a neurotransmitter.
- It is produced in stressful situation, increase heart rate and blood flow.
- Leading to physical boost and heightened awareness.
- Nor-adrenaline (concentration) : It improve attention and responding actions in the brain. Contracts blood vessels, increasing blood pressure.
- Dopamine (pleasure) : Feeling of pleasure, also addiction, movement and motivational.
- People's repeat behaviours lead to dopamine release.
- Serotonin (mood) : Contributes to well beings and happiness. Helps sleep cycle and digestive system regulation.
- GABA (Calming) : Calm firing nerves in the CNS. High level improve focus. Low level cause anxiety. Also contributes to motor control and vision.
- Histamine : Released by mast cells, involved in local immune responses. Contraction of smooth muscle tissue of the lungs, uterus and stomach.
- Glutamate (memory) : Involved in learning and memory. It regulates development and creation of nerve contacts.
Drugs acting on Autonomic Nervous System
These all are those drugs which act on Autonomic Nervous system and produce effect on it.
- Adrenergic drugs [sympathomimetics] Sympathetic Nervous system
- Antiadrenergic drugs [Sympatholytics] Sympathetic Nervous system
- Cholinergic drugs [Parasympathomimetics] Parasympathetic system
- Anti-Cholinergic drugs [Parasympatholytics] Parasympathetic system
What we have to study??
- Introduction/Defination
- Synthesis, storage, Release, Degradation
- Receptor and Mechanism
- Classification / Drugs Name examples
- MOA (Mechanism of Action)
- Uses
- Blocking Agents and Pharmacological action.
CHOLINERGIC SYSTEM
Also known as Parasympathomimetics system.
Parasympathomimetics
- Parasympatho Parasympathetic Nervous system
- mimetic (mimic) copy the action.
- These are those chemical agents or drugs which copy the action of parasympathetic Nervous System.
- These drugs bind with cholinergic receptors [Muscarinic & Nicotinic] and give their action.
Why??
- When the neurotransmitter of parasympathetic nervous system (Acetylcholine) in body is less as per demand, then we use drugs externally which act as cholinergic neurotransmitter. i.e.. parasympathomimetics.
eg. Acetylcholine, Neostigmine, Physostigmine etc.
Pharmacological action of parasympathomimetics
- i) Cardiovascular System ($M_2$ receptor)
- depress auricular muscles
- contraction of bundle of his Av node
- BP due to vaso dilation.
- ii) Eye
- Constrict the pupil and cause miosis.
- Intraocular pressure decreases.
- used in Glaucoma.
- iii) Skeletal muscles
- Contraction of skeletal muscle.
- useful in myasthenia gravis.
- iv) Respiratory system
- Bronchoconstriction.
- Induce Asthma.
- v) Gastrointestinal system
- Contract smooth muscle of GIT.
- increase tone, motility and peristalsis movement.
- Increases salivary, pancreatic, Liver, gall bladder and Intestinal secretions.
Therapeutic uses
- Glaucoma (physostigmine, Pilocarpine)
- Myasthenia gravis (Neostigmine)
- Paralytic ileus and Post-operative Urine retention (Bethanechol, Carbachol)
- Atropine poisoning (Physostigmine)
- Curare poisoning neuromuscular Junction block (Neostigmine)
- Alzheimer's disease (cholinesterase Inhibitor)
Adverse effects : Parasympathomimetics may cause-
- Nausea
- Vomiting
- Bradycardia/Hypotension (higher doses)
- Cause Asthma
Parasympatholytics
- Parasympatho parasympathetic Nervous System
- Lytics lysis (breakdown) Oppose the effect
- These are those drugs which inhibit the effect of acetylcholine or parasympathomimetics by blocking the cholinergic receptors.
Pharmacological action of Parasympatholytics (Atropine)
i) CNS : It can cross BBB (Blood brain barrier) so it can produce their effect in CNS.
- It cause respiratory depression.
- It cause drowsiness and sedative effects.
ii) Cardiovascular system : It block receptors and cause
- increase the heart rate
- Increase the conduction from SA node.
iii) Eye :
- Cause mydriasis
iv) Exocrine gland :
- Decrease secretion of salivary, bronchial, gastric, pancreatic, lacrimal and sweat gland.
- rise in body temp.
v) GIT :
- Reduce motility of GIT.
- Gastric juice secretion reduced.
- Used to treate peptic ulcer.
Therapeutic uses
- mydriatic
- Anti-parkinsonism agent
- Pre-anaesthetic medication
- Motion sickness
- peptic ulcer
- Bronchial Asthma [Ipratropium]
- Anti-cold tablets.
Adverse effects may cause
- can cause glaucoma in some patients.
- Tachycardia
ADRENERGIC SYSTEM
It involves sympathomimetics drugs
Sympathomimetics
- Sympatho Sympathetic Nervous System
- Mimetics mimic (copy the action)
- These are those chemical agents or drugs which copy the action of sympathetic nervous system.
- These drugs bind with adrenergic receptors [Alpha & Beta] and give their action.
- eg. Adrenaline [Epinephrine], Nor-adrenaline [Nor-epinephrine], Phenylephrine etc.
Pharmacological action of sympathomimetics (Adrenaline)
i) Cardiovascular system
- increase force of contraction.
- Increase in Heart rate.
- Increase in Cardiac output.
- Blood vessels on skeleton muscles vasodilation.
- Blood vessels on smooth muscles, Heart, coronary arteries vasoconstriction.
ii) Respiratory system
- on receptor Bronchodilation
- receptor present in the blood vessels of nasal mucosa. cause vasoconstriction of nasal mucosa.
iii) Eye ($\alpha_1$ receptor)
- Contraction of radial muscle of iris Cause mydriasis dilation of pupil of the eye.
iv) GIT (Gastro intestinal tract)
- Relaxation of GI smooth muscles.
v) Urinary tract
- Relaxation of urinary bladder ($\beta_2$) and closure of sphincture ($\alpha_1$).
- Urinary retention.
Therapeutic effects
- Bronchial asthma (Salbutamol)
- Nasal decongestant
- As a cardiac stimulant in case of sudden Cardiac arrest.
Adverse effects
- Restlessness
- Anxiety
- Insomnia
- Blood pressure
- Contra-Indicated in:
- Hypertension
- Diabetes
- Arteriosclerosis.
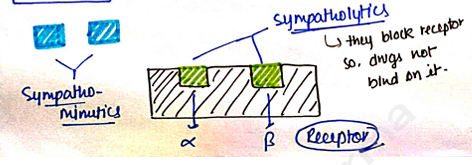
Sympatholytic
- Sympatho Sympathetic Nervous System
- Lytic (lysic) Oppose (breakdown)
- These are those drugs which inhibit the effects of sympathomimetic drug by blocking the receptor.
- Also known as
- Anti-adrenergic drugs
- Adrenergic antagonist
- Adrenergic blocker.
pharmacological action of sympatholytics
- blockers vasodilation and BP.
- blockers stimulates release of Nor-adrenaline tachycardia. $\alpha$-blockers produce Hypotension, tachycardia, Increased cardiac output.
- blockers decrease heart rate.
- blockers cause Bronchoconstriction.
- blockers block lipolysis & glycogenolysis.
Therapeutic uses
- i) \alpha$-blockers $\rightarrow Hypertension, Congestive heart failure, Peripheral vascular disease,
- ii) \beta$-blockers $\rightarrow Angina pectoris, Myocardial infarction, Cardiac arrhythmias, Glaucoma.
NEUROMUSCULAR BLOCKING AGENTS
SKELETAL MUSCLE RELAXANTS (peripheral)
Neuromuscular blocking agents
These are those agents or drugs which are used to block the Neuromuscular Junction (NMJ) and inhibit the contraction of muscle and cause relaxation of muscles. They are also known as Skeletal muscle relaxants.
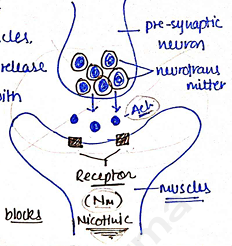
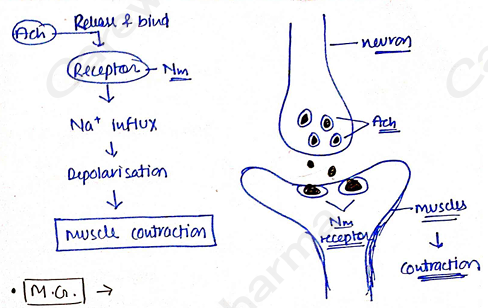
Neuromuscular Junction (NMJ)
- It is the Junction b/w the neuron and muscles.
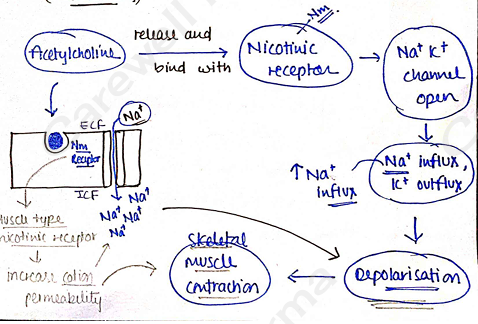
- in which, neurotransmitter release from neuron and bind with nicotinic receptor present on muscle and cause contraction & movement.
- Neuromuscular blocking agent blocks this NMJ.
Uses
- generally used by Doctor for relaxation of muscle during operation.
- used to improve symptoms such as muscle spasm, pain and hyperreflexia.
- used as a alternate of anaesthetic.
General procedure of muscle contraction (mechanism)
Classification
Skeletal Muscle Relaxants (Peripheral)
Non-depolarizing (competitive) blockers
- Long acting: d-Tubocurarine, Pancuronium, Doxacurium, Gallamine triethiodide.
- Intermediate acting: Atracurium, Vecuronium, Rocuronium.
- Short acting: Mivacurium.
De-polarizing blockers
- Succinylcholine [Sch]
- Decamethonium
1) Non-depolarizing blockers
- The first neuromuscular blocking drug was Curare - Used by south american hunter to paralyse the animals.
- Most used d-tubocurarine [d-TC].
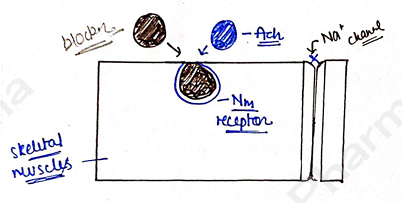
Mechanism
- They are competitive antagonist and structural analogs of acetylcholine.
- Tubocurarine and other non-depolarizing blockers have quaternary compounds with positively charged nitrogen.
- So, they have affinity to bind (Nicotinic) receptor but have no intrinsic activity.
- Acetylcholine and these blockers fight for one place (receptor) and finally these blockers bind with receptor in place of acetylcholine.
- Therefore, the motor nerve impulse connot transmit and contraction is stopped (prevent).
- Finally, skeletal muscle relaxation occurs.
Pharmacological action
i) skeletal muscles : induced flaccid paralysis. paralyse acc to this order: muscles of face eye finger limb neck trunk. recovery occurs in reverce order.
ii) Histamine release : d-TC has a greater tendency to liberate histamine from mast cells.
iii) Cardiovascular system :- d-TC produce hypotension due to histamine release. Gallamine cause tachycardia.
iv) Respiratory effect : Bronchospasm.
v) Autonomic ganglia : produce some degree of ganglionic blockade.
- It can overcome or reverse by use of Neostigmine and Pyridostigmine which increase the availability of Ach (increase concentration) by inhibiting Acetylcholinesterase (enzyme).
Adverse effect
- Hypoxia
- Respiratory paralysis
- Hypotension
- Constipation
- Tachycardia etc--
2) Depolarizing blockers
- there are non-competitive antagonist.
- Mostly used succinylcholine (Sch) as general clinical use.
- Succinylcholine does not hydrolyzed by Acetylcholinesterase.
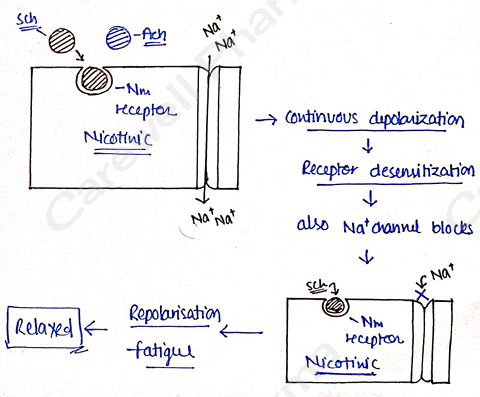
Mechanism
- They have similar action as acetylcholine.
- But Sch does not hydrolyzed or terminate.
- In case, when Ach bind on receptor, it cause depolarisation but after some time Ach hydrolysed by cholinesterase enzyme normal sufficient response (contraction) Relaxed.
Pharmacological action
- muscle twitching
- muscle soreness
- Apnoea.
Therapeutic uses
- initial ingredient
- adjuvants to general anaesthesia.
- prevent trauma during electroconvulsive therapy.
- to control ventillation.
Adverse effects!-
- muscle rigidity
- prolonged apnoea
- Nausea & Vomitting.
- Muscle soreness.
- Example! Succinylcholine (Sch), it can degrade by butyrylcholinesterase.
LOCAL ANAESTHETICS
Basic terms
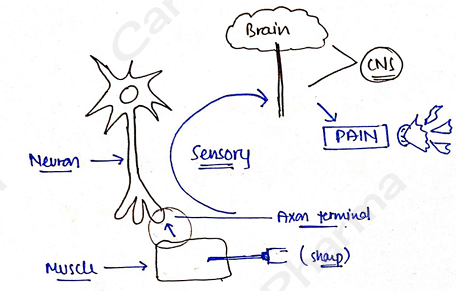
Pain : A symptom of being hurt or sick. OR unpleasant Sensation.
It Can be mild discomfort but sometime it is out of control.Sensation : It is a feeling which you feel when you come in contact with anything. (hot, cold, soft, hard).
Analgesic : Those drugs which reduce pain and produce analgesia effect. Used as a painkiller.
Anaesthetic : Those drugs which reduce Sensation which further reduce pain.
Reversible loss of sensation. (sensation back after some time/work).Local anaesthetics : loss of sensation & pain at any particular area OR a local area. used for a minor surgery. eg. removal of tooth, eye surgery etc. Drugs: Lidocaine, Procaine etc.
General anaesthetics : Loss of sensation in complete full body. used for a major operation/surgery eg Heart surgery, organ transplant etc. Drugs: opioids, diazepam, isoflurane etc.
Definition
- These are those drugs which blocks the neuronal conduction at any particular area in body.
- they produce reversible loss of sensation.
- also cause muscular paralysis.
Classification
Surface
- Soluble Cocain, Tetracaine, Lidocaine
- Insoluble Benzocaine, Oxethazain
Injectable
- Low potency / short duration procaine, chloroprocaine.
- Intermediate potency / duration Lidocaine, Prilocaine.
- High potency / long duration Tetracaine, Ropivacaine.
Injectable anaesthesia :
- Those drugs which inject under the skin (not through I.V.).
- Used for minor surgery
- Skin cut etc. eg Procaine, Bupivacaine etc.
- All types of local anaesthetic drugs contain tertiary amine structure. So, they are basic in nature.
- They are lipophilic in nature, so they can easily cross membrane (mostly).
- L.A. contain two types of bond
Amide bond : Lidocaine, Bupivacaine, tetracaine etc.
Ester bond : procaine, cocaine, Benzocaine etc.
Surface anaesthesia : Apply topically on skin. Sensory nerve ending are affected. Limited to surface (mucous) membrane. It can damaged skin surface, wound or burns. eg. Benzocaine, Lidocaine etc.
Mechanism of Action
1) Normal (Resting condition) : When no impulse generate no sensation. m-gate (close).
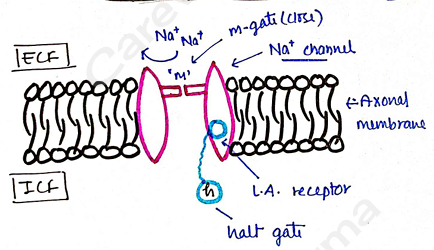
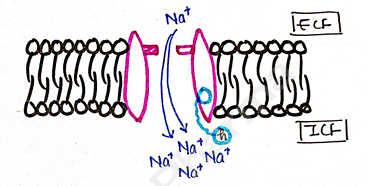
- 2) Activated : Any signal (impulse) generate m-gate open channel open ion influx Depolarisation Sensation OR Response.
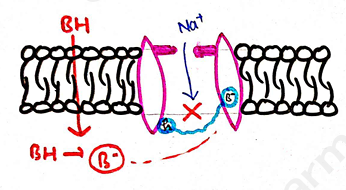
- 3) Inactivated :
- Now, L.A. drugs introduced into body (BH).
- which can easily cross membrane (axonal).
- Now in intracellular it dissociate into ionized form .
- Now, bind with LA receptor which close (block) the channel with the help of halt(h) gate.
- Depolarisation stop Loss of sensation. Reversibly.
Adverse effects
- Tounge numbness
- Muscle twitching
- Hypotension
- Redness of skin
- Asthma
Uses
- Loss of sensation (reduce pain).
- nerve block (block voltage gated channel).
- Used as ointment, injection etc.
DRUGS USED IN MYASTHENIA GRAVIS
Myasthenia Gravis
A weakness and rapid fatigue of muscle.
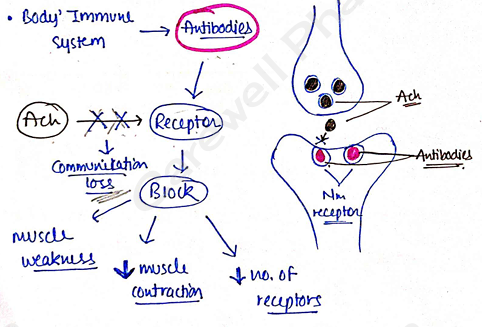
- It is an auto-immune disorder, in which our immune system produce antibodies that block or destroy muscle's receptor.
- Breakdown in communication b/w nerves and muscles.
Symptoms
- weakness in the arms and leg muscles.
- Double vision.
- Difficulties with speech and chewing.
- fatigue, shortness of breath.
Mechanism
- Normal : When myasthenia gravis not occurs and our body behave normal and contraction and relaxation happened normally in muscles.
- M.G. :
- It is an auto-immune disorder.
- In this disorder, our immune system produce antibodies to block/destroy the Nicotinic receptor.
- Because, Acc to Immune system these receptors are harmful for body.
- So, these antibodies bind with these receptor and block them.
- Now due to blockage of receptor, acetylcholine (Ach) does not bind on receptor.
- Due to this, there are loss of communication b/w nerves (Ach) and muscle.
- Which further decrease the contraction of muscles. Also muscle become weak & fatigue.
- These antibodies also destroy or kill the receptor. Due to this there are also decrease in the no. of receptors.
TREATMENT
Drugs Used.
1) Anticholinesterase
- Use these drug to treate myasthenia gravis.
- Anticholinesterase drugs inhibit cholinesterase enzyme. cholinesterase inhibit the acetylcholine by hydrolysis.
- So, when these drugs inhibit (stop) these enzymes, concentration of Ach Increases. By Ach release can replace antibodies.
- eg. Pyridostigmine, Neostigmine etc.
2) Immuno suppresant :
- Use these drugs to suppress the immune system to decrease the formation of antibodies.
- eg Cyclosporine A, Methotrexate, Azathioprine, Cyclophosphamide etc.
3) Corticosteroids :
- Decrease Antibodies.
4) Plasmapheresis (plasma exchange) :
- It is a technique used to treat myasthenia gravis.
- the plasma of the blood is exchange with substitute plasma, so Antibodies (Ab) remove from body and immune system does not attack the body's own tissue.
- Increase synthesis of nicotinic receptor.
DRUG USED IN GLAUCOMA
Glaucoma
A group of eye condition that can cause blindness (loss of vision).
- In this, the nerve connecting the eye to the brain (optic nerves) is damaged due to high eye pressure (intra ocular pressure).
- Intra-ocular pressure is more than 21 mmHg.
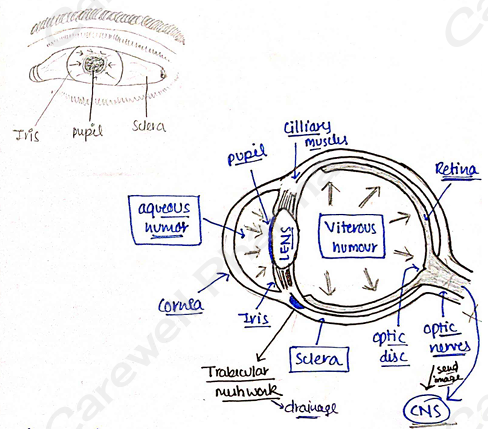
- two main reason:
- production of aqueous humour
- drainage of aqueous humour
- I.O.P. damage eye optic nerve Loss of Vision (Blindness).
Symptoms
- eye pain
- mid-dilated pupil
- redness of the eye
- Vision loss, blurred vision
Risk factor
- Increased pressure in the eye
- Due to genetic factor (family history)
- High blood pressure
- Excessive use of liquid diets (such as alcohol etc).
- Excessive use of steroids
Diagnosis
- Dilated eye examination.
Types
- 1) Open angle glaucoma
- Also known as chronic and wide angle glaucoma.
- production of aq. humor > drainage of aq. humor.
- symptoms: gradual vision loss, Optic nerve damage.
- 2) Angle closure glaucoma
- most common type of glaucoma.
- Also known as acute and narrow angle glaucoma.
- flow of Aqueous humor blocked drainage Severe Quick painfull increase in pressure an emergency condition.
- Symptoms: severe pain, Nausea, Blurred vision.
Treatment
By I.O.P (Intraocular pressure)
i) $\alpha$-agonist I.O.P by increasing the Uveoscleral outflow. drainage of aq. humor. eg. Brimonidine, Apraclonidine, Dipivefrine etc.
ii) $\beta$-blocker I.O.P by decreasing the formation of aq. humor. eg. Timolol, Betaxolol, Levobunolol etc...
iii) Prostaglandin (P.G.) analogues I.O.P by Uveoscleral outflow. Same as $\alpha$-agonist. eq. Latanoprost, Travoprost, Bimatoprost etc.
iv) Carbonic anhydrase inhibitors used orally. aqueous formation by bicarbonate ion in ciliary epithelium. eg. Acetazolamide, Dorzolamide.
v) Miotic agent I.O.P by increasing ciliary muscle tone. (used rarely for glaucoma). eq. Pilocarpine etc..