Pharmacology 1 - Unit 1
Syllabus
1. General Pharmacology
- Introduction to Pharmacology- Definition, historical landmarks and scope of pharmacology, nature and source of drugs, essential drugs concept and routes of drug administration, Agonists, antagonists( competitive and non competitive), spare receptors, addiction, tolerance, dependence, tachyphylaxis, idiosyncrasy, allergy.
- Pharmacokinetics- Membrane transport, absorption, distribution, metabolism and excretion of drugs .Enzyme induction, enzyme inhibition, kinetics of elimination
Scroll to Download
PHARMACOLOGY-I
GENERAL PHARMACOLOGY
UNIT- 1ST
INTRODUCTION TO PHARMACOLOGY
Pharmacology : To study about the drugs. $\downarrow$ pharmacon + logy (Drug/medicines) + (to study)
Pharmacology = Pharmacodynamics + Pharmacokinetics
- It is the branch of science with deal with the study of pharmacodynamics and pharmacokinetics.
- It is all about study of drug and effect of drug on body and body's response for the drugs.
Pharmacodynamics
- The branch of pharmacology concerned with the effect of drugs and the mechanism of their action.
1. Pharmacodynamics
Pharmaco + Dynamics (Drug Effects)
- What does drug do to the body.
- Mechanism of drug action to the body.
Pharmacokinetics
- Te branch of pharmacology concerned with the movement of drugs within the body.
2. Pharmacokinetics
- What does body do to the drug.
- ADME
- A = Absorption
- D = Distribution
- M = Metabolism
- E = Elimination
GENERAL PHARMACOLOGY
Historical landmarks and scope of Pharmacology
Introduction to Pharmacology - Definitions
Pharmacology : It is the branch of science which deal with the study of uses, effects and mode of action of drugs.
Clinical Pharmacology : Study of drugs with their clinical uses.
Drug : A medicine or other substance which give therapeutics effect when ingested into body.
Pharmacokinetics : It is branch of pharmacology concerned with the movement of drug in body. study about (ADME) absorption, distribution, metabolism and excretion of drug in body [What body does to the drug].
Pharmacodynamics : It is branch of pharmacology concerned with the effect of drugs on body. (what does drug do to the body).
Toxicology : The branch of science concerned with the study of poisons, toxic substances and their antidote or treatment.
Chemotherapy : It is the branch in which we study about the Use of chemical drugs for the disease (effect of drugs).
Adverse drug reaction : In pharmacology, any unexpected or dangerous reaction to a drug. An unwanted effect caused by the administration of a drug.
Bioavailability : It is defined as "The rate and extent to which the active substance is absorbed from a pharmaceutical form and becomes available at the site of action."
HISTORICAL LANDMARKS
- The knowledge of drugs and their uses for diseases are as old as history of mankind.
- Primitive man (Ancient) gather the knowledge of healing and medicines by observing the nature, noticing the animals while ill and personal experience after consuming plants and herbs as remedies.
- They discovered that extracts from plants, animals and minerals had medicinal effects on body.
LANDMARKS
Hippocrates (460-375 BC) : A greek physician consider "FATHER OF MEDICINES". He was the first person who recognize disease as abnormal reaction of body. He introduce use of metallic salts for the treatment of disease.
Paracelsus (1493-1541) : Grand father of pharmacology. He introduces the use of chemicals for treatment of disease.
MODERN PHARMACOLOGY
Oswald Schmiedeberg (1838-1921)
FATHER of PHARMACOLOGY
He established pharmacology as an independent discipline.
Estimation of chloroform in blood.John Jacob Abel (1857-1938)
Isolation of histamin from pituitary.
Preparation of pure crystalline Insulin.Paul Ehrlich (1854-1915)
Paul Ehrlich was a Nobel Prize-Winner.
FATHER OF CHEMOTHERAPY.
find a cure for syphilis in 1909. (used arsenical for Syphilis).Alexandar Fleming (1881-1955)
Scottish physician.
He discovered world's first broadly effective antibiotic substance which he named Penicillin.Ramnath Chopra (1882-1973)
He was an Indian Medical service officer (IMS).
FATHER OF INDIAN PHARMACOLOGY.
Systemetic study of Indian Medicinal plant.
SCOPE OF PHARMACOLOGY
- Study about pharmacokinetics, what does body do to the drug [ADME].
- Study about pharmacodynamics, what is the effects of drug to the body.
- So, In present time there are many scopes in pharmacology such as Research, Industries and academics etc..
- Clinical pharmacology, in which we study about both desirable and undesirable effects of drug. Contraindication of drugs, their Bioavailability and also about posology (dose).
- Study of toxicology (study toxic substances and their actions, then antidote and prevention/treatment).
- Study about drugs which is use for the disease or disorder which is comes under pathophysiology.
- Study of forensic science (investigating).
- Their are also great scope of pharmacology in research such as Drug discovery and Drug development, Clinical trials.
- Drug discovery for new drugs.
- Drug development development of new drugs.
- On clinical trials (according to their phase). first pre-clinical trials (drugs applied on animals) then second trials for humans if suitable or pass in pre-clinical trials.
Pharmacogenomics : It is use of genetic information to guide the choice of drug & dose. It helps in drug discovery and minimize adverse drug reaction.
Pharmacogenetics : It is study of genetic basis for variability in drug response, it also helps in development of drugs.
NATURE AND SOURCES OF DRUGS
Nature of drugs
All drugs are chemical entities with simple or complex molecules.
- Inorganic drugs : Some drugs are of inorganic nature. eg Ferrous Sulphate, Lithium carbonate etc.
- Organic drugs : Majority of drugs are organic compounds.
- it may be
- weakly acidic (aspirin, penicillin) or
- weakly basic (morphine) or
- non-electrolytes (alcohols etc).
- it may be
- Mostly drugs are normaly solids, eg Paracetamol, ampicillin etc.. but some such as ethanol, glycerol are liquids, and few like nitrous oxide are gaseous.
- The molecular weight of majority of drugs in the range of 100-1000D.
According to their action
- Preventive - Those drugs which used to prevent the cause of the disease.
- Symptomatic - Those drugs which used to treate the symptom of that disease.
- Diagnostic - Those drugs which helps to determine the causes of disease.
- Curative - Those drugs which used in treatment of any disease.
- Health Maintainance - Those drugs which help to maintain our health.
SOURCES OF DRUGS
i) Plants
ii) Animals
iii) Microbes
iv) Minerals
v) Synthetic
vi) Biotechnology.
i) Plants : Many plants contain biologically active substances and are the oldest sources of drugs.
eg - Tulsi (used for cough treatment & cold remedies)
Neem (antimicrobial activity)ii) Animals : Though animal parts have been used as cures since early times.
eg. - Thyroxine, insuline, liver extracts (Vit. B12).- Used for making vaccines (blood).
- Used of insulin for control diabetes.
iii) Microbes : Most antibiotics are obtained from fungi, bacteria etc...
eg - Penicillin, tetracycline etc.- Some times vaccines are also produced by the use of microbes.
iv) Minerals : Their are many more minerals which is used as a medicinal substances.
eg - Iron (Anemia), Zinc (wound healing), Iodine (Antiseptic), Silver (Immunity booster) etc...v) Synthetic : It is the largest sources of medicines.
It has the advantages of purity and uniformity of the product, they can be manufactured as per need.
eg - fluoroquinolones, Bismuth iodine etc.vi) Biotechnology : In which, combined biological organism with technology to generate new drugs.
eg. - Peptides & proteins are now produced by recombined DNA technology.- Human growth hormone
- Human Insulin etc.
Essential Drug Concepts and Routes of drug administration.
Essential Drug Concept
- WHO (World Health Organization) introduced the concept of essential medicines (drug) in 1977. [included 208 medications].
Definition
"These are those drugs which satisfy the priority health care needs of the population"
Criteria
They are selected with due regard to
- Public health relevance.
- Clinical evidance on efficacy and safety.
- Comparative cost effective (individual & community can afford).
- Available at all time in adequate amount and appropriate dosage form.
- Assured quality and adequate information.
India proposed its first list in 1996, has revised it in 2003, 2011, and now in April 2015 with the title name "National list of essential medicines" [includes 376 medicines].
- The WHO updates the list in every two years.
- It can be differ from country to country due to change in their environment.
eg : Paracetamol, Acetylsalicylic acid [Aspirin], Ibuprofen etc. for pain and palliative care relieving pain.
- Activated charcoal Used as a antidote (used in poisonings).
Routes of Drug administration
"A route of administration in pharmacology is the path by which a drug/medicine or any other substance is taken into the body."
Classification
On the basis of their location, they can be classified as:-
- Local
- Topical (on skin)
- Inhalation (Nasal)
- Rectal/vaginal
- Auricular [Ear]
- Systemic
- Enteral
- Oral
- Sublingual*
- Buccal*
- Rectal*
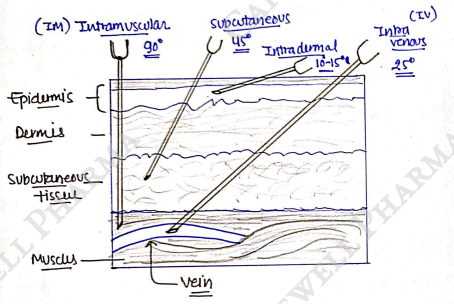
- Parenteral
- Intravenous (IV)
- Intramuscular (IM)
- Subcutaneous
- Intradermal
- Intra cardiac
- Intra arterial
- Inhalation/Nasal*
- Enteral
Local Routes of drug administration
It is the simplest route, in which drug is applied only on a particular area or directly on a site of action.
- Topical route In this, drug is applied externally on the surface of skin and give localized action.
- advantages: Apply for local action, more convenient as well as encouring to patient. painless, safe, cheap, useful for childs.
- disadvantages: Slow action, some drugs cause irritation.
Drug can be efficiently delivered to the localized lesion on skin, in the form of lotion, ointment, cream, powder, sprays etc..
- Inhalation/Nasal It also a part of systemic circulation, in which drug is inhaled through mouth/nose and gives their action on an particular area and also some drug is absorbed in blood through blood capillaries present in mucosa/muscles (rapid absorption & effects).
eg. Asthma used as a bronchodilators.
- Rectal/Vaginal In which, special types of drug preparation is injected into rectum and vagina to give their local action on it.
eg. Suppositories or Enema etc.- advantages: given to unconscious patients. Ideal if drug cause vomiting.
- disadvantages: cause irritation, not a well accepted route.
- Auricular (ear) / eyes / nasal cavity In this, drug is introduced into body cavity like ear, eye, and produced a local effect in it.
eg : drops, ointment and sometimes suspensions.
SYSTEMIC ROUTES
In which, the drug administered through systemic routes means absorbed into the blood stream and distributed all over including the site of action.
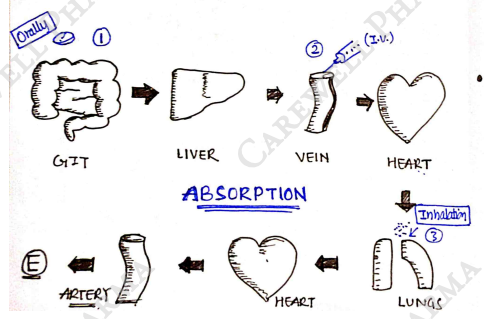
- Enteral It means through instestinal (GIT). In which drug pass through intestine then reach into blood.
It show first pass metabolism.
first pass metabolism : In which drug directly goes into liver after intestine through portal vein, in which drug metabolise and their bioavailability will be decrease.
Oral route: It is the oldest and simplest method (route) for drug administration.
In which drugs is directly swallow through mouth and it reach in systemic by passing GIT.
Both Solid dosage form (powders, tablets, capsules, etc.) and Liquid dosage form (elixirs, syrups, emulsions etc) can be given orally.advantages: Safe, more convenient, does not need assistance, Painless, cheap & cost effective, Easily available.
disadvantages: Slow responses due to first pass metabolism. not suitable for emergencies.
- Parenteral : (par-Beyond, enteral-intestinal) In this drug is reaches into blood stream other than intestinal routes.
It follow Bypass metabolism.
Bypass metabolism : In which drug directly (absorb) reaches into blood then reach at site of action through circulation without passing intestine & liver.
i). Sublingual/Buccal route : It may be in the part of enteral. The tablet or pellet containing the drug is placed under the tongue/crushed in the mouth and spread over the mucosa, which further absorbed into the blood.
Only lipid soluble drug can be administrated also it is non-irritating.advantages : rapid action, it follow bypass metabolism.
disadvantages: Inconvenient for patient.
eg : GTN, buprenorphine etc.
ii). Intravenous (IV):
Subcutaneous : Drug is deposited into loose subcutaneous tissue, which is richly supplied by nerves.
advantages: Action of drug are uniform.
Self-injection possible due to less penitration.disadvantages: Avoided in shock patients.
Absorption is slower than intramuscular.
iii). Intramuscular (IM) : The drug is injected into muscles, then drug reach into blood circulation. Injection inject at a angle of .
advantages: By pass metabolism (rapid response).
Useful for unconscious patients.disadvantages: Small dose.
Mild irritant on be cause irritation.
v). Intradermal : The drug is injected into the skin raising a blub (a small blister on the skin).
Injected into epidermis/dermis.
Rarely used (only for specific purpose).
eg. BCG Vaccine.
vi). Intracardiac : Drug is directly injected into muscles of heart.
It is only used in an emergency situation.
Need an expert for this.
vii). Intra arterial : Drug administrate into artery (blood vessels that carries blood from the heart to the tissue & organs).
Anti-cancer drug can be injected through it.
Important Terms in Pharmacology
- Agonists
- Antagonists (competitive and non-competitive)
- Spare Receptors
- Addiction
- Tolerance
- Dependence
- Tachyphylaxis
- Idiosyncrasy
- Allergy
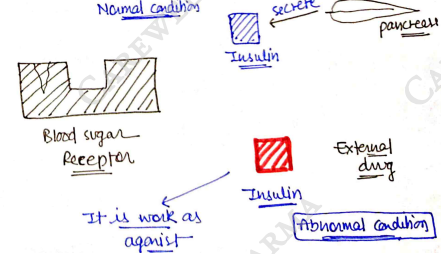
1) Agonists - "These are those drug/substance that binds to a receptor and cause the same pharmacological action as the substance that normally binds to the receptors" It can be:
- full agonists - high efficacy, full response
- inverse agonists - opposite response
- partial agonists - lower efficacy, less response
Normal condition: Pancreas secrete Insulin Blood sugar Receptor. Abnormal condition: External drug Insulin (It is work as agonist) Receptor.
eg : Heroin, Methadone, Mophine [all are full etc...]
Terms
- Receptor: those binding sites in which drug attach, then activate it and give a pharmacological action.

- Efficacy: ability of drug to bind.
- Potency: Action (response) by drug.
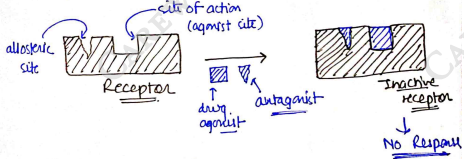
2) Antagonists - "These are those drug/substance which has similar structure like agonist and bind with receptor but they do not give any pharmacological action instead they block the receptor and inhibit the agonists/natural substance to bind with receptor."
- It is of two types
i) Competitive
ii) Non Competitive
i) Competitive : "These are those antagonist which have similar structure like agonist." It can block receptor 100%. so their efficacy is 100%. OR It inhibit the full response of agonist.

There are a competition between antagonist and agonist, by increasing the concentration of agonist can overcome competitive antagonist activity. eg. Morphine Naloxone.
ii) Non-Competitive antagonist: "these are those antagonist which bind to an allosteric (non-agonist) site of the receptor to prevent activation of the receptor."
- They have different structure than agonist.
3) Spare Receptor - "These are those receptor which are not occupied by the drug molecules to produce 100% response"
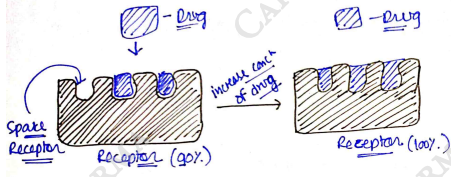
eg. receptor (occupied only 90% drug) of Heart. In emergency situation (such as heart failure) occupied 100% receptor and give more pharmacological action.
- Addiction "Specific side/adverse effect of drugs caused by prolonged use"
- When we take any drug/substance for a long duration, then it show some unusual response in our body.
- It is a psychological & physical inability to stop consuming drug even doing cause harm.
- It is considered as brain disorder.
eg. Heroin, Cocain, Alcohol etc.
- Tolerance : "It is the diminished effect (response) of any drug, when drug give repeatedly for long duration in the same dose."
- It happens when a person no longer responds to a drug in the way they did it first. So it takes a higher dose of the drug to achieve the same effect as when the person first used it.
eg. excess use of paracetamol etc.
- It happens when a person no longer responds to a drug in the way they did it first. So it takes a higher dose of the drug to achieve the same effect as when the person first used it.
- Dependence : When a person take any drug/substance for a long duration for any reason/cure, then our body become dependent on that drug and behave normal with that drug.
- If body not receive that drug, then it may cause Headache, Nausea, discomfort etc.
Diagram: Body + Drug Normal; Body without drug Abnormal headache etc.
eg. excess use of paracetamol. excess use of Analgesics drug used to relieve pain (painkillers).
- If body not receive that drug, then it may cause Headache, Nausea, discomfort etc.
- Tachyphylaxis : "Rapid decrease in the response of drug upon repeated administration of same dose in short intervals". also known as acute tolerance.
eg : Ephedrine, Nicotine etc.
- Idiosyncrasy : It is a condition in which a unusual effect such as side effect of any drug is seen only in very less population (or a particular people). these effects known as idiosyncratic effects.
eg. Barbiturate (CNS depressant), but it cause some side effect such as mental confusion & excitement in some peoples.
- Allergy (Drug allergy) : Some drugs/substance cause the unwanted side effect or adverse effect to our body.
"An abnormal reaction of the immune system to a medication/drug."
eg. Ibuprofen, Aspirin etc. most common form of allergic reaction are skin reactions such as rashes, itching etc.
PHARMACOKINETICS
- Pharmacokinetics is the quantitative study of drug movement in, through and out of the body.
- "What does body do to the drug".
- It involves four processes [ADME]:
- Absorption
- Distribution
- Metabolism
- Excretion
1) ABSORPTION
"It is defined as the movement of drug molecules from its site of administration to the systemic circulation."
- It is first and important step of pharmacokinetics. when we take any drug through oral route, it goes into stomach in which disintegrate and dissolution take place, then drug reach into intestine.
- Now, after dissolution drug absorb into blood through membrane.
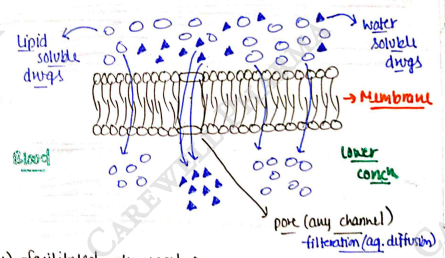
Membrane : It is a biological membrane, which made up with phospholipids and cholesterol and other groups (bilayer).
- It act as a semipermeable membrane.
- Now, Drug reaches into systemic circulation through membrane transport.
Which are following :
i) Passive transport
ii) Active transport
iii) Facilitated transport
iv) Endocytosis
Concentration gradient : when any drug/substance move from high concentration to lower concentration.
i) Passive transport : Also known as passive diffusion.
- In this transport, drug/substance move across the concentration (high to low).
- Most of the drug are absorb by passive diffusion. diffusion across the cell membrane. Osmosis through semi-permeable membrane. Lipid soluble drugs cross membrane.
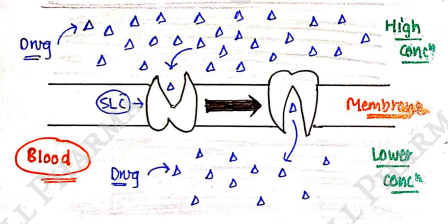
ii) Facilitated transport : In this transport, drug molecules move across the concentration gradient, but with the help of any carrier bodies.
- Some large molecules or poorly diffusible substance does not passes through passive transport,
- So they required help of any carrier body to cross the membrane.
- Carrier such as SLC (solute carrier transporter).
iii) Active transport : In this transport, drug molecules move against the conc gradient [Low High].
- It required energy due to movement of drugs against the conc gradient. ATP is used (ATP hydrolysis ADP).
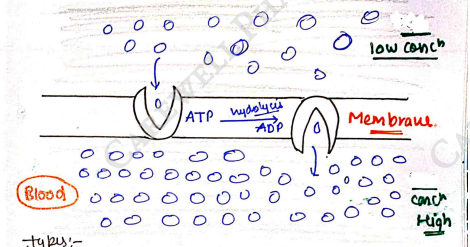
Types
- primary through energy (ATP) eg. Na-K pump. Secondary antiporter & symporter pump etc.
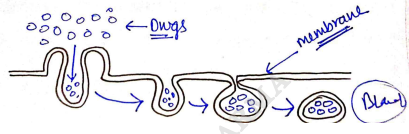
iv) Endocytosis : In this transport, drugs of very large size get transport via engulfment by cell membrane.
- Due to large size, they do not cross membrane and also not fit in any channel.
- Absorption is not exactly straight forward (simple), it is a variable process, depend on various factors:
- Factor Affecting Drug Absorption
1) Physio-chemical properties
i). Particle size (drug molecules)
ii). Formulation (dosage form)
iii). Ionisation
iv). pH
v). Lipid solubility & Concentration
2) Biological Factor
i). Surface area
ii). Membrane transport
iii). Gastric emptying time
iv). Blood flow (circulation)
v). Food
3) Routes of administration [Bioavailability & First pass mutabolism]
Physio-chemical properties
i) Particle size (drug molecules) : It is inversely proportional to the absorption.
Particle size .
- The smaller the particle size, the greater will be its absorption because small size drug particles dissolve easily.
ii) Formulation (dosage form) : In solid, Liquid,
parenteral (Injection). Parenteral > Liquid dosage form > solid.
iii) Ionisation : We all know that, both form (ionised + unionised) are important for pharmacological response of drugs. But, for absorption drug must be in unionized formed.
iv) pH : It tell about nature of drug (Acidic/Basic). Acidic drug must absorbed in stomach. Aspirin. Basic drug must absorbed in intestine. Morphine.
v) Lipid solubility : lipophilic nature's drug has slightly higher absorption than hydrophilic, because in membrane transport Lipid soluble drug cross membrane easily.
vi) Concentration : we know that passive diffusion follow conc gradient, so higher the conc of drugs, the greater will be its absorption.
Biological factor
i) Surface area : Area of absorbing surface.
- It is directly proportional to the absorption.
Surface area Absorption.
So, the larger (greater) the surface area for absorbing drug, the greater will be its absorption.
ii) Membrane transport : Most of the drug absorb through passive diffusion, because it does not require energy or anything, and also follow conc gradient.
Passive transport > facilitated > Active transport.
iii) Gastric emptying time : Those drugs whose gastric emptying time is more (fast), their rate of absorption is high.
- But time is not too fast, otherwise drug is excrete without absorption. So it is at optimum time.
iv) Blood flow (circulation) : directly proportional. the more blood flow in body, the greater will be absorption of drug.
v) Food : It will also affect the absorption of drug. If the food is present inside the stomach, then it dilute the drug and absorption will be decreases.
- So, take medicine after some time of meal.
Route of administration
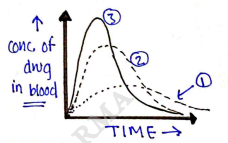
This affects drug absorption, because each route has its own peculiarities
- Route of administration affect the bioavailability of drugs.
Bioavailability : Total amount of drug which reach into the systemic circulation.
- Parenteral route has maximum bioavailability (drug absorb maximum).
- In I.V. (intravenous), drug directly release into blood. so their absorption & bioavailability is 100%.
- In Subcutaneous/intramuscular, drug injected near the capillaries also have great absorption & bioavailability.
- Enteral (oral) has less bioavailability & absorption, because it follow first pass metabolism (drug passes through liver which decrease the absorption).
2) Distribution
After Absorption, drug reach into systemic circulation [Blood].
Drug distribution : The movement of drug from Systemic circulation to interstitial fluid (extracellular fluid) and various other part of body.
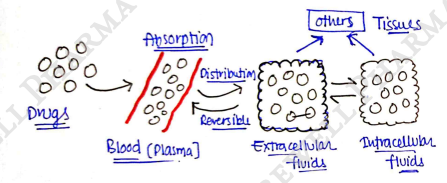
- It is a passive diffusion process H L.
- Drug distribute non-uniform throughout the body.
- It is a reversible process.
Factor affecting drug distribution : Distribution is very important step of pharmacokinetics, because in which drug reach to site of action then bind with receptor and give pharmacological action.
It is also depend on many factors:-
i). Blood Flow
ii). Lipophilicity
iii). Capillary Permeability
iv). Plasma protein binding
v). Some other factors
i) Blood flow : Where will be more blood flow, there will be more distribution.
high blood flow Brain, Heart, kidney, Liver etc... [Distribution \uparrow$]. Low blood flow $\rightarrow skeletal muscle, Adipose tissue etc. [Distribution $\downarrow$].
ii) Lipophilicity : Greater the Lipid solubility of the drugs, faster is its distribution. Because membrane is Lipophilic, so drug can easily cross. Lipophilicity = Distribution .
iii) Capillary permeability : The higher the permeability of capillary, the greater will be the distribution of drugs. (eg. Liver , Brain Distributing). It is depends upon Barriers (Physiological barriers):
- Barriers (Physiological barriers)
1) BBB (Blood-Brain barrier) The Capillary endothelial cells in brain have tight junction & lack space (pores), and investment of neural tissue cover the capillaries.
Both forms BBB.
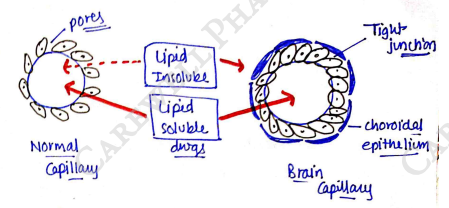
- these barrier are Lipoidal, so only Lipophilic (Lipid soluble) drug distributed.
2) BCSFB blood-CSF-barrier, same as BBB.
3) Blood Placenta Barrier (BPB) It is seen in pregnancy, which protect foetus.
- It is also Lipoidal and allow Lipophilic drugs, and restrict hydrophilic.
- But sometime it not work on drug taken by mother can affect the foetus/newborn.
- Nature : lipid soluble drug has high permeability so great distribution.
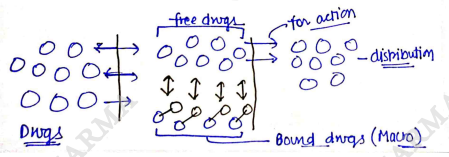
iv) Plasma protein binding : When drug reach into systematic circulation, then their are two form of drug:
- Free drug & Bound drug (those drug which bind with plasma protein).
- Most of the drug bind with albumin.
eg : Acidic drug generally bind to albumin.
Basic drug generally bind to $\alpha_1$-acid glycoprotein. - Bound drug (plasma protein bound drug) has less distribution, because their size increase (Macro) so they can not cross easily membrane.
- Free drug has good distribution. eg Barbiturates bound with albumin. Methadone bound with $\alpha_1$-acid glycoprotein.
v) Others :
- Age - also affect distribution, due to different in total body weight, fat content etc...
- Obesity, high adipose tissue can take up large fraction of lipophilic drug.
- Redistribution - distributed drug again distributed. eg. Brain/heart/kidney/Liver distributed drug Muscle/fat etc.
Volume of distribution
apparent volume of distribution.
It help to know about the distribution of drug in body fluids, throughout the body.
3) Metabolism
Also know as biotransformation.
- The conversion of drug from one chemical form to another.
- Aim To convert Lipid soluble (non-polar) drug to water soluble (polar) drug to avoid reabsorption in renal tubules and help in excretion. (remove the drug from body).
- Lipid soluble (Active drug) Water soluble (Inactive form of drug). (increase polarity).
- Inactive drug (pro drug) Active form.
- eg. morphine morphine-6-glucuronide (active metabolite).
- Most of the drug are lipid soluble (lipophilic), so it can be easily excreted out through metabolism. But some drug are hydrophilic (eg. Streptomycin, neostigmine etc.) are less bio-transformed and excreted unchanged.
- Metabolites: The drug which convert after metabolism.
Drug Phase-I (Oxidation, Hydrolysis, Reduction) Metabolites-A excrete through kidney - Metabolites-A Phase-II (conjugation) Metabolites-B Excretion through Urine (kidney) & Bile
- The primary site for drug absorption / metabolism is liver and others are kidney, intestine, lungs and plasma. There are different kinds of enzyme system present in liver (highest), smooth endoplasmic reticulum of the liver and also in other organs such as kidney, lungs etc... but in smaller conc. which biotransform the drug molecules. mostly biotransformation are done by microsomal enzymes such as Cytochrome P-450, Oxidase, glucuronyl transferase.
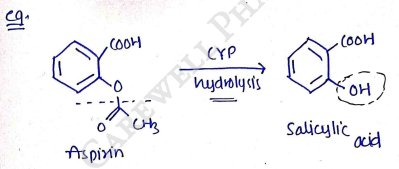
1) Phase-I reaction : In this, the drugs can be metabolized by Oxidation, reduction, hydrolysis and increase polarity of drugs so drug can easily excrete from kidney.
- These are non-synthetic reaction.
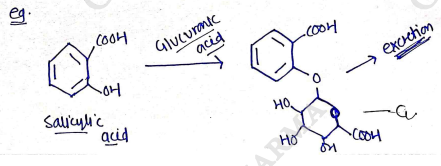
2) Phase-II reaction :- (Synthetic reaction)
- It is faster than phase-1 and also those not excreted after phase-I can excreted through phase-II.
- It involves conjugation with an endogenous substance such as glucuronic acid, sulfate, glycine.
- These reaction are more polar, so drug can easily excreted by the kidney & liver (bile).
Factor affecting drug metabolism including
i) chemical factor
a) Enzyme induction : The phenomena of increased drug metabolizing ability of enzymes by several drugs & chemicals known as enzyme induction & agents called enzyme inducers.
- It is due to
- increase in both liver size & liver blood flow.
- increase stability of cytochrome P-450 enzymes.
eg. Rifampin Induction of CYP3A4 Contraceptic steroids Inactive, Eliminated).
b) Enzyme inhibition : A decrease in the drug metabolizing ability of an enzyme is called as enzyme inhibition. direct interaction at the enzyme site & change enzyme activity [Comp. & Non-Comp.]. Indirect due to fall in rate of enzyme synthesis (repression) or due to nutritional deficiency or hormonal imbalance (altered physiology).
e.g. Erythromycin, Ketoconazole Inhibition of CYP3A4 Terfenadine Active antihistamine.
ii) Biological factor
a) Age : The drug metabolic rate is different in different age groups.
- neonates (upto 2 month) & infants (2m-1year) metabolism - slowly (due to less development of microsomal enzyme).
- children (1yr-12yr) metabolism - Rapid as compared to adults.
- elderly person metabolism - slowly .
b) Diet : The enzyme content and activity is altered (affected) by dietary components.
eg low protein diet slowly metabolism. high protein diet rapid metabolism. because protein diet increase enzyme synthesis.
c) sex difference : It also affect drug metabolism.
eg Benzodiazepines - metabolize slow in women than men. metabolize rapid in men than women. there are also some factor which affect metabolism such as hormonal imbalance, Pregnancy, diseases, etc..
iii) Physicochemical properties pKa, solubility, polarity, size, shape etc.. also affect the drug metabolism by interaction with the active sites of enzymes.
iv) stereochemical aspects It also affect drug metabolism, because some metabolizing enzyme often display a preference for one enantiomer of a drug over the other (enantioselectivity).
It is due to differ in their action. D(+) glucose easily metabolised than L(-) glucose (not metabolised).
4) Elimination
Excretion of drugs It is the removal of systemically absorbed drug from our body. It is the last step of pharmacokinetics.
Routes of elimination
Urine : Most of the drug are excreted through the kidney by the process of urination. Water soluble drug (hydrophilic drug) excreted out through this. (hepatic renal)
Faeces : Some of the drug in liver is absorbed in bile (which is secreted in liver) which further excreted through faeces. Mostly lipid soluble drug (lipophilic) excreted through this. eg Erythromycine etc.
Lungs (exhaled air) : some drugs in form of gas and volatile liquids are eliminated through exhalation by lungs. General anaesthetics, alcohol.
Sweat & Saliva : Some of drug is excreted in the form of sweat from skin. Some drug excreted through sputum which is mix with saliva, but most drug which along with saliva go into oral route. Lithium, heavy metals etc. - minor excretion.
Milk : In pregnant or new mother women's, some drugs enter breast milk by passive diffusion, and then excreted through mother's milk. Lipid soluble & less protein bound drug excreted through this.
Kinetics of Elimination
Clearance (CL) : "The clearance of a drug is the theoretical volume of plasma from which the drug is completely removed in a unit time".
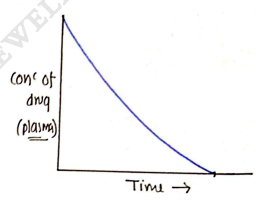
First order kinetics : The amount of drug eliminated over time is directly proportional to the conc of drug in body.
Rate of elimination drug concentration.
In this, drug eliminated at constant rate, e.g., 15%, but the amount of drug (mg) is changed.
Most of the drug is eliminated through first order kinetics.
- Zero order kinetics : The amount of drug eliminated is independent of drug conc.
Rate of elimination = Constant. eg. Aspirin, Alcohol, Lithium etc.
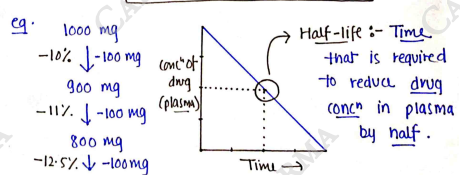
- Half-life:- Time that is required to reduce drug conc in plasma by half.